Dear Fellow Physicians,
Opposition to Maintenance of Certification (MOC), once again remains a top national medical news story. Nationwide, physicians from most specialties are expressing their views on the pitfalls and merits of Board Recertification and MOC. As of this update, it has surpassed 20,000 signatures against MOC. It is one issue that has physicians across the country unified on - petition after petition, starting with the original one from Change Board Recertification in 2010, to Dr. Paul Teirstein’s in 2015, to the current petition by Dr. Aaron Goodman. The frustration against MOC isn’t new.
It started with one physician who had been diligently practicing medicine for many years and realized how onerous and outrageous MOC and recertification had become. That physician writes a letter to the NEJM, creates this website that remains to this day the repository for information about MOC. Since then physicians have been vocalizing their concerns. The response is loud and clear – end MOC.
Although the National Board of Physicians and Surgeons (NBPAS) has become a valid and sustainable board to maintain certification and has been accepted by nearly 200 hospital systems, MOC is still required by academic institutions and large health systems like HCA.
NBPAS meets national accreditation standards for health plans and hospitals including National Committee on Quality Assurance (NCQA), Utilization Review Accreditation Commission (URAC), Center for Improvement in Healthcare Quality (CIHQ), Accreditation Commission for Health Care (ACHC) and was named as a “Designated Equivalent Source Agency” by The Joint Commission (TJC).
Physicians took political action in multiple states and have drafted resolutions and legislation in opposition to MOC and Maintenance of Licensure (MOL). And the MOC story even went mainstream with four major articles in Newsweek.
Multiple anti-trust lawsuits against ABMS member boards have been filed by Practicing Physicians of America and Association of American Physicians and Surgeons.
As it stands, it’s been mostly SILENCE from ABMS and its member boards, but most of us who have been putting in the time and effort for over a decade at the grassroots level are not surprised.
While the vast majority of physicians want MOC abolished, we feel that the system's self-evaluation of medical knowledge modules can function as a worthy alternative to CME—but only if universal lifetime board certification is restored and the extortion and pressure associated with MOC compliance are eliminated. Our responsibility for continuing education credits should be no different from those of other licensed professions - remain up-to-date with CME requirements and in good standing in the community without the further burden of imposed regulations or testing requirements.
We take issue with the bulk of the MOC process: Modules and Patient and Peer Reviews amount to little more than busy work, and the costly, time-consuming Secure Examination—which requires an enormous amount of preparation and time off from work —is clinically irrelevant and has no place in the life of a practicing physician.
Of course, these criticisms are sticking points for our Boards, which derive income directly from this part of MOC. In fact, the ABIM claims it makes no money from MOC and that its members receive a minimal stipend to attend meetings and write exam questions—yet each such question costs $4,000 (through "stringent psychometric testing”), the ABIM President makes a salary of about $2,000 a day, and the costs associated with the MOC program since 2006 have inflated the ABIM’s revenue to $149,800,000—a number which grows yearly and with each modification to MOC.
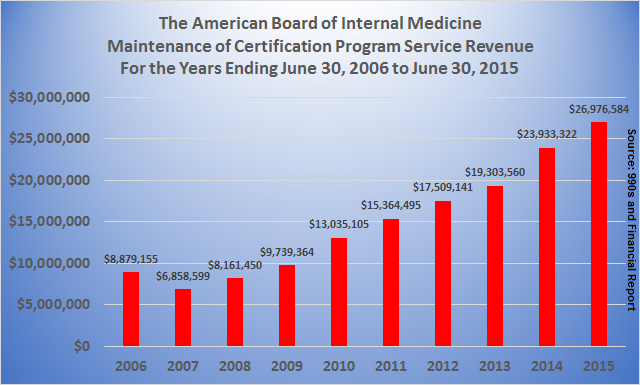
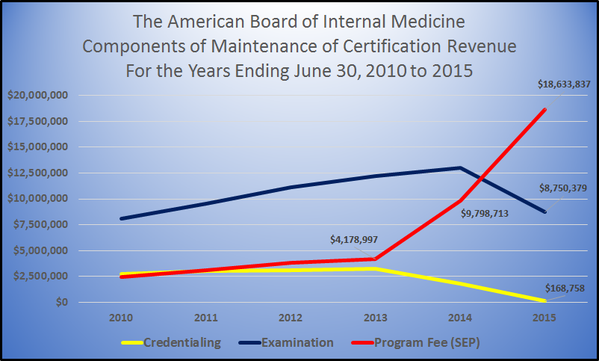
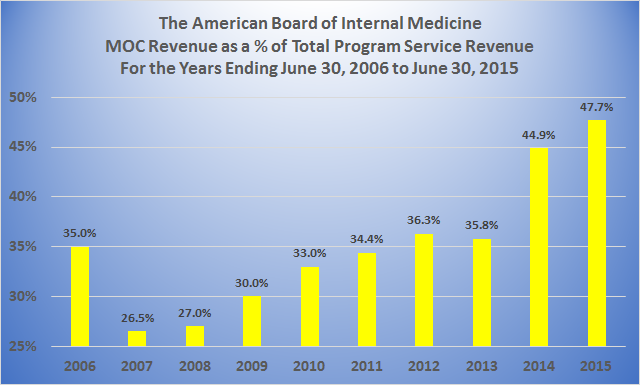
Review these five graphs below for a breakdown on the ABIM's finances. And for more eye-opening tax return and financial information about the ABIM and all the Boards, please click here on "The Boards - Tax Returns" .
In ten years MOC Revenue has tripled from $8.9 million in 2006 to $27 million in 2015, resulting in increased revenue for the ABIM by $149,800,000 . . .
In two years the SEP portion of MOC Revenue has quadrupled from $4.2 million to $18.6 million . . .
MOC Revenue now represents 47.7% of ABIM's total revenue . . .
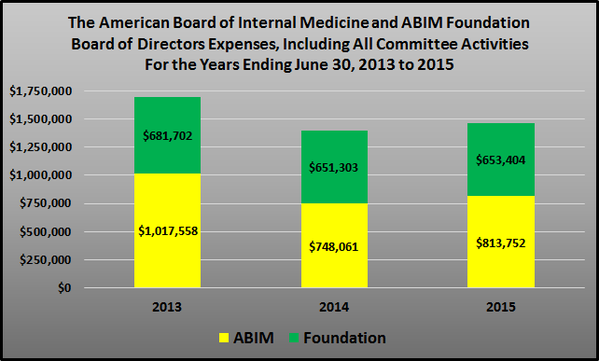
For the last three years the ABIM and ABIM Foundation has incurred Board of Director Expenses of $4.6 million . . .
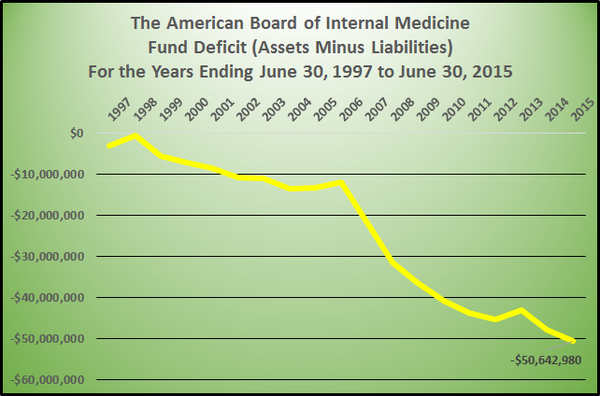
Yet despite all this increased revenue from MOC, as of June 30, 2015 the ABIM's fund deficit (assets minus liabilities) has somehow plummeted to minus $50.6 million . . .
We are all for staying current with medical changes, but the onerous MOC program is no way to achieve this. It's a money-making juggernaut with scant data to support any benefit for improving physicians' skills or ensuring patient care and safety. And it lacks reasonable financial transparency.
If the ABIM, ABMS and FSMB have their way, MOC (soon to become CMOC, or Continuous MOC) will become an every-two-year cycle—which, according to the ABIM, will "simplify and streamline the process" and ultimately be tied into Maintenance of Licensure (MOL).
We need to act collectively. The number-one disease afflicting physicians is apathy, and it's the main reason our profession is trouble.
Our goals remain clear:
- 1. MOC should not be associated with hospital privileges.
- 2. MOC should not be associated with insurance reimbursements or network participation.
- 3. MOC should not be required for Maintenance of Licensure.
- 4. MOC should not be mandatory.
- 5. All Board certificates must be converted to lifetime status; only then will MOC be voluntary.
Please click on all links and review the rest of our website. Educate yourself. Get involved in your community and at the state level, and forward this website to all your colleagues.
It's imperative that each physician get involved in the following manner:
- 1. Organize with colleagues to petition your hospital to eliminate MOC as a requirement for maintaining your hospital privileges.
- 2. Do the same with your individual boards, as they are already collaborating with health plans to base reimbursement on MOC requirements.
- 3. Approach your city and state medical organizations, as they are attempting to tie MOC to MOL.
- 4. Just say no to MOC. Should you feel a need to continue certifications, consider switching to the National Board of Physicians and Surgeons (www.NBPAS.org).
Remember: MOC + MOL = BIG TROUBLE. If MOC gets tied to MOL, it is no longer voluntary; it becomes mandatory.
It's clear that Board leadership ignores its constituency, so follow the steps as outlined above and continue to pressure your board into radically simplifying or scrapping MOC. Also support the Association of American Physicians and Surgeons (www.aapsonline.org), who have already filed suit against the ABMS.
MASS MOC NONCOMPLIANCE is the only rational solution to forces taking over our profession.
But it will to take all of us have an impact.
Please get involved. Feel free to share ideas at this site or "Join The Discussion" for ongoing discussions on SERMO and LinkedIn
Thank you again for your support.